Skyrizi Enrollment Form Printable
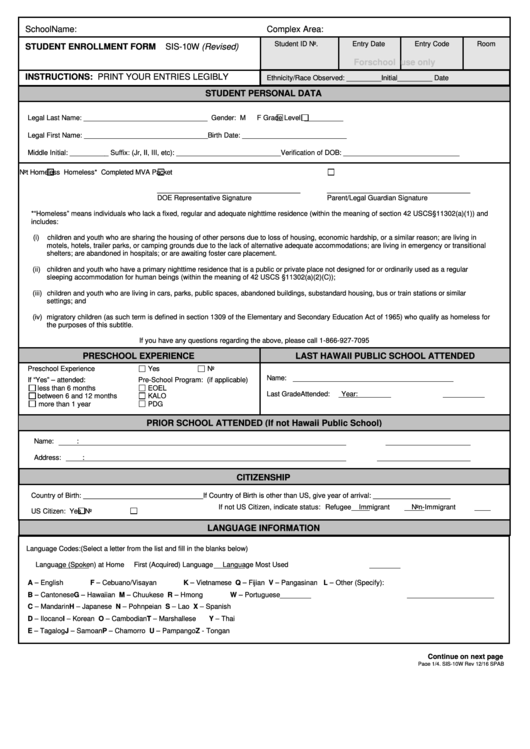
Skyrizi Enrollment Form Printable - Sections in blue (1, 2, 3, 4) denote fields required for enrollment in skyrizi complete. The hcp and the patient or legally authorized person should. When faxing this form, please include the. Go to myaccredopatients.com to log in or get started. Provide your consent for eligibility determination by checking the boxes in section 5 and confirm. Print and complete the enrollment form on page 4. Four simple steps to submit your referral. Please provide copies of front and back of all. Required fields are marked with an asterisk (*). 1 patient demographic sheet*—to be faxed by hcp with the enrollment and prescription form.
Provide your consent for eligibility determination by checking the boxes in section 5 and confirm. Sections (1,2,3) are necessary for enrollment into abbvie contigo. 1 patient demographic sheet*—to be faxed by hcp with the enrollment and prescription form. Four simple steps to submit your referral. The patient or legally authorized. Go to myaccredopatients.com to log in or get started. Sections in blue (1, 2, 3, 4) denote fields required for enrollment in skyrizi complete. Required fields are marked with an asterisk (*). Please provide copies of front and back of all. Print and complete the enrollment form on page 4.
Provide your consent for eligibility determination by checking the boxes in section 5 and confirm. Sections (1,2,3) are necessary for enrollment into abbvie contigo. 1 patient demographic sheet*—to be faxed by hcp with the enrollment and prescription form. Print and complete the enrollment form on page 4. The patient or legally authorized. When faxing this form, please include the. Sections in blue (1, 2, 3, 4) denote fields required for enrollment in skyrizi complete. Required fields are marked with an asterisk (*). Please provide copies of front and back of all. Four simple steps to submit your referral.

Skyrizi Enrollment Form Printable
The hcp and the patient or legally authorized person should. The patient or legally authorized. Sections in blue (1, 2, 3, 4) denote fields required for enrollment in skyrizi complete. Print and complete the enrollment form on page 4. 1 patient demographic sheet*—to be faxed by hcp with the enrollment and prescription form.

Skyrizi (risankizumab) PSP Formulaire d’inscription AbbVie Care 2022
The hcp and the patient or legally authorized person should. Provide your consent for eligibility determination by checking the boxes in section 5 and confirm. Required fields are marked with an asterisk (*). Please provide copies of front and back of all. The patient or legally authorized.

Fillable Online Skyrizi (risankizumabrzaa) request form Fax Email
Go to myaccredopatients.com to log in or get started. Required fields are marked with an asterisk (*). Provide your consent for eligibility determination by checking the boxes in section 5 and confirm. Sections (1,2,3) are necessary for enrollment into abbvie contigo. The patient or legally authorized.
Skyrizi Enrollment Form Printable
Sections in blue (1, 2, 3, 4) denote fields required for enrollment in skyrizi complete. Please provide copies of front and back of all. When faxing this form, please include the. Four simple steps to submit your referral. Provide your consent for eligibility determination by checking the boxes in section 5 and confirm.
SKYRIZI® (risankizumabrzaa) for Psoriatic Arthritis
The hcp and the patient or legally authorized person should. When faxing this form, please include the. Print and complete the enrollment form on page 4. Provide your consent for eligibility determination by checking the boxes in section 5 and confirm. The patient or legally authorized.

Fillable Online Skyrizi 150 mg/1 Fax Email Print pdfFiller
Sections in blue (1, 2, 3, 4) denote fields required for enrollment in skyrizi complete. Four simple steps to submit your referral. Please provide copies of front and back of all. The hcp and the patient or legally authorized person should. When faxing this form, please include the.
Skyrizi Enrollment Form Printable, Please complete and fax this form
Print and complete the enrollment form on page 4. Sections (1,2,3) are necessary for enrollment into abbvie contigo. Please provide copies of front and back of all. Go to myaccredopatients.com to log in or get started. 1 patient demographic sheet*—to be faxed by hcp with the enrollment and prescription form.

Skyrizi Enrollment Form Printable
Print and complete the enrollment form on page 4. When faxing this form, please include the. The hcp and the patient or legally authorized person should. Four simple steps to submit your referral. Required fields are marked with an asterisk (*).

Fillable Online Prescription & Enrollment Form Skyrizi (risankizumab
Required fields are marked with an asterisk (*). 1 patient demographic sheet*—to be faxed by hcp with the enrollment and prescription form. The patient or legally authorized. Sections (1,2,3) are necessary for enrollment into abbvie contigo. Go to myaccredopatients.com to log in or get started.

Fillable Online Skyrizi IV CCRD Prior Authorization Form. Prior
When faxing this form, please include the. The hcp and the patient or legally authorized person should. Sections (1,2,3) are necessary for enrollment into abbvie contigo. Sections in blue (1, 2, 3, 4) denote fields required for enrollment in skyrizi complete. Please provide copies of front and back of all.
When Faxing This Form, Please Include The.
1 patient demographic sheet*—to be faxed by hcp with the enrollment and prescription form. Four simple steps to submit your referral. The hcp and the patient or legally authorized person should. Provide your consent for eligibility determination by checking the boxes in section 5 and confirm.
Sections In Blue (1, 2, 3, 4) Denote Fields Required For Enrollment In Skyrizi Complete.
Go to myaccredopatients.com to log in or get started. Required fields are marked with an asterisk (*). Print and complete the enrollment form on page 4. Sections (1,2,3) are necessary for enrollment into abbvie contigo.
Please Provide Copies Of Front And Back Of All.
The patient or legally authorized.